Sat, Apr 27, 2024
[Archive]
Volume 27, Issue 4 (October 2023)
2023, 27(4): 211-218 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Sadeghi R, Omidi F, Raoufi M, Hassanpour R. Comparing Clinical Parameters and Outcomes of ST-elevation Myocardial Infarction (STEMI) Patients With and Without COVID-19 Infection. Hormozgan Medical Journal 2023; 27 (4) :211-218
URL: http://hmj.hums.ac.ir/article-1-38-en.html
URL: http://hmj.hums.ac.ir/article-1-38-en.html



Department of Clinical Pharmacy, Faculty of Pharmacy, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
Full-Text [PDF 536 kb]
(76 Downloads)
| Abstract (HTML) (209 Views)
Full-Text: (23 Views)
Introduction
The novel coronavirus disease 2019 (COVID-19) emerged in Wuhan, China, in December 2019, rapidly evolving into a global pandemic. During the COVID-19 pandemic, the incidence of cardiovascular diseases, including acute coronary syndromes (ACS), stress-induced cardiomyopathy, arrhythmias, and myocarditis, increased [1].
Several mechanisms have been proposed for the pathogenesis of COVID-19 in myocardial injuries. These mechanisms include cytotoxic effect and endothelial damage by angiotensin–converting enzyme 2 (ACE-2) receptor expressed in the myocytes, coronary microvascular obstruction owing to hyperinflammation and prothrombotic state, a mismatch of myocardial supply and demand due to cytokine storm, and acute respiratory distress syndrome (ARDS) associated hypoxemia [2, 3].
The COVID-19 outbreak negatively influences admission rates and the reperfusion strategy for patients with ST-elevation myocardial injury (STEMI) worldwide [4]. Declining admission rates of STEMI patients with COVID-19 and a delay in symptom onset to first medical contact or door-to-balloon have been reported in this population [5, 6]. Additionally, the definition and diagnosis of STEMI in COVID-19 cases have been complex and challenging due to factors such as social distancing, lockdown, health care burden due to the COVID-19 pandemic, and unclear diagnosis of heart attack [4, 5].
Objectives
We designed this study to compare the characteristics, management, and clinical outcomes of patients with STEMI with and without COVID-19.
Materials and Methods
Settings and study population
This prospective observational study was conducted on adult patients diagnosed with STEMI at the Imam Hossein Medical Center, affiliated with Shahid Beheshti University of Medical Sciences (SBMU) in Tehran City, Iran, in the first 6 months of the pandemic, spanning from February 2020 to August 2020.
Assessments
All enrolled patients were evaluated for COVID-19 infection based on reverse transcription polymerase chain reaction (RT-PCR), typical clinical features, and computerized tomography (CT) scan results. Also, STEMI was defined according to the universal definition of myocardial infarction (MI) [7]. All infected patients were managed according to standard treatment protocol based on the updated World Health Organization (WHO) guideline treatment.
Patients were divided into two groups: COVID-19-positive and COVID-19-negative. Then, they were monitored during hospitalization and 6 months after discharge by telephone call. The study data, including baseline characteristics, comorbid risk factors, drug history, clinical and laboratory data, and outcomes, were recorded and compared between the two groups.
Statistical analysis
All statistical analyses were performed using SPSS software, version 21 for Windows (SPSS Inc., Chicago, IL, USA). A P<0.05 was considered statistically significant.
Quantitative data were tested for normality by the Kolmogorov-Smirnov test and then compared by the unpaired t and Mann-Whitney U tests for normally and non-normally distributed data, respectively. Qualitative data were analyzed by the chi-squared or Fisher exact test. The data were presented as Mean±SD or median (percentile, Q1, Q3) for normal and non-normal distributed quantitative data, respectively, and n (%) for qualitative data.
Results
During the period of the study, 131 patients were admitted with STEMI. of whom, 29 patients (22.13%) were diagnosed with COVID-19. None had an RT-PCR result at admission, but they had typical clinical features and CT scan results of COVID-19 infection.
All patients underwent primary angioplasty upon admission, except for 12 patients who initially received thrombolytic treatment (10 and 2 in the COVID-19-negative and -positive groups, respectively; P=0.632), but some hours later, some were candidates for rescue percutaneous coronary intervention (PCI) due to cardiogenic shock (4 patients), persistent chest pain (5 patients) and non-acceptable ST resolution (3 patients).
Most patients were men in two groups of the study (82.35% and 58.62% of COVID-19-negative and -positive, respectively; P=0.007). Also, there was a statistically significant difference between the two groups regarding age, and COVID-19-positive patients were older (63.97±12.54 vs 58.19±10.97 years, P=0.039). Data are presented in Table 1.

The COVID-19-positive patients exhibited a higher prevalence of diabetes (P=0.003) and heart failure (P=0.008). Still, the two groups had no statistical differences for the other comorbid risk factors or drug history (Table 1).
Table 2 presents severe symptoms, echocardiographic and angiographic findings, and some laboratory data during admission.
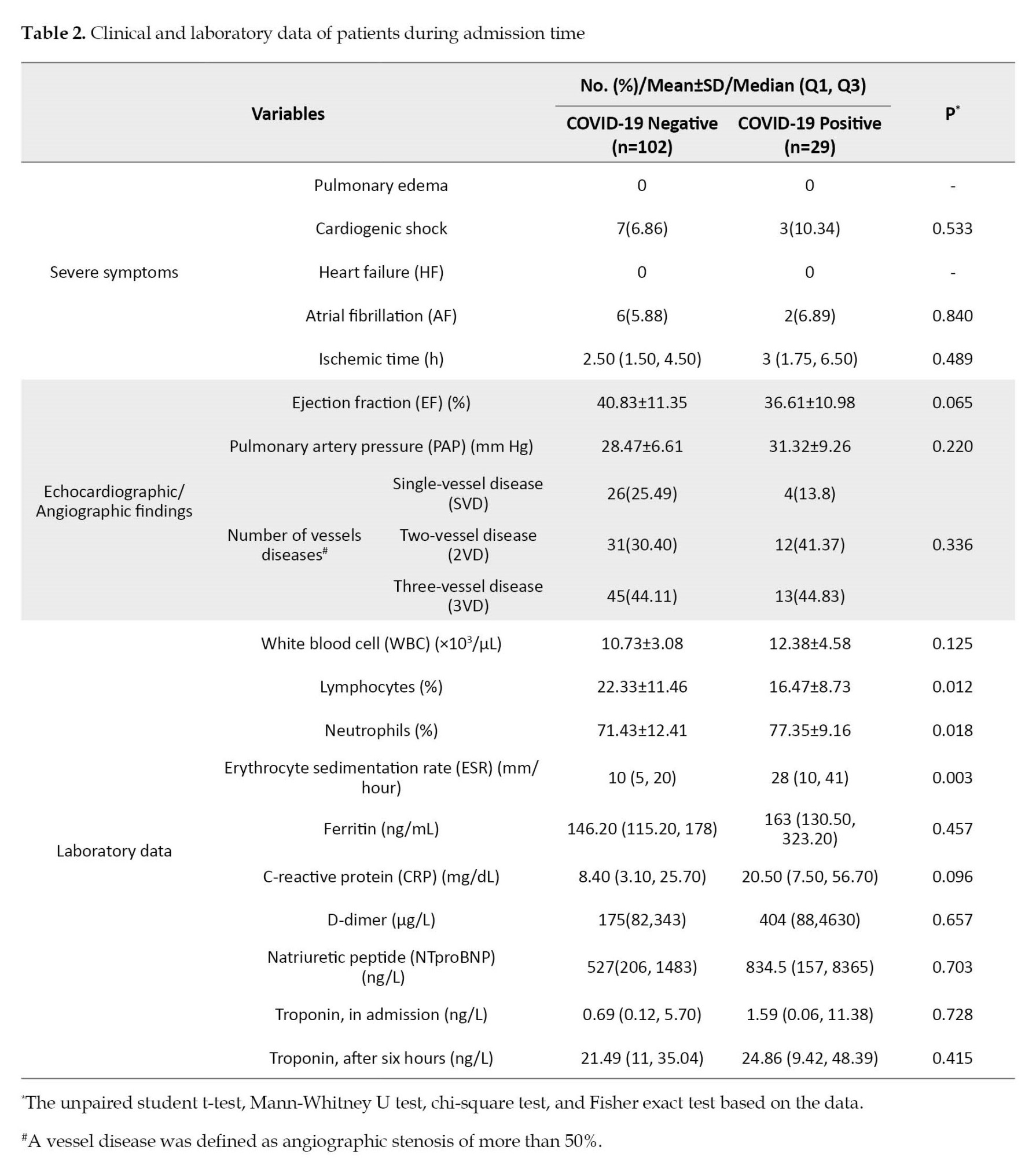
Erythrocyte sedimentation rate (ESR) and neutrophil count were significantly higher in STEMI patients with COVID-19 infection (P=0.003 and P=0.018, respectively). Instead, lymphocyte count was significantly declined in COVID-19-infected patients (P=0.012).
Whereas STEMI patients with COVID-19 infection were more frequently subjected to coronary artery bypass graft (CABG) surgery during the first admission time (6.7% COVID-19-positive vs 1.96% COVID-19-negative), but this difference was not statistically significant (P=0.173). Furthermore, there were no statistical differences in other complications during hospitalization between the two groups of the present study (Table 3).

In addition, hospital length of stay (HLS) was statistically higher in the patients concomitant with COVID-19 infection (6.64±4.30 vs 4.93±3.59 days; P=0.023).
There were no statistically significant differences between the two groups regarding mortality rate during hospitalization (P=0.095) and 6 months after discharge (P=0.978). During the study period, the overall mortality rate in our setting was 8.82% and 17.24% in COVID-19-negative and -positive, respectively. There was also no statistically significant difference between the two groups (P=0.195). The results are reported in Table 4.

Discussion
This study evaluated clinical characteristics and outcomes in STEMI patients comorbid with COVID-19 infection. We described our healthcare system’s experience of patients presenting with STEMI during the first 6 months of the COVID-19 pandemic. Primary angioplasty is the best-recommended therapy for STEMI, and our setting is an academic center with 247 primary angioplasty and a success rate of more than 95% [8].
Cardiovascular diseases and underlying comorbidities have a high prevalence among COVID-19 patients. Increased risk and severity of COVID-19 infection were also proven in patients with comorbidities [1, 9, 10]. This finding accords with our observations, which showed that the comorbidities, including hyperlipidemia, hypertension, diabetes, chronic kidney disease (CKD), chronic obstructive pulmonary disease (COPD), heart failure, and cerebral vascular accidents (CVA) were common in COVID-19 positive groups. However, only diabetes and heart failure were significantly more frequent in the STEMI patients with confirmed COVID-19.
Furthermore, prior studies have noted that many admitted patients with COVID-19 were men. Evidently, male gender and advanced age were independent risk factors for mortality in the COVID-19-positive population [11, 12]. Consistent with the noted literature, most patients in our study were men, and those infected patients with COVID-19 were older.
Inflammatory markers such as ESR, C-reactive protein (CRP), ferritin, and D-dimer have increased, but lymphocyte levels and neutrophilia are decreasing in COVID-19-infected patients [13]. In addition, Case et al. evaluated natriuretic peptide (NTproBNP) in acute myocardial infarction (AMI) patients with and without COVID-19 infection, which was increased in patients with COVID-19 [9]. In our setting, the patients with COVID-19 had higher levels of WBC, neutrophil, ESR, CRP, ferritin, D-dime, and NTproBNP. However, this study found no significant difference between inflammatory markers except ESR, lymphocyte, and neutrophil.
The present study did not show any significant increase in mortality rate among patients with concomitant COVID-19. This outcome is contrary to that of Case et al., who found a significantly increased mortality in AMI COVID-19-infected patients compared with AMI patients without COVID-19 [9].
The decline in the number of hospital admissions of patients with STEMI because of various reasons such as society’s fear, lockdown, and allocation of high capacity of the hospital for COVID-19 patients during the early months of the pandemic contributed to the small sample size in our study. Therefore, the low sample size and the unequal number in the two study groups are possible reasons for these statistically non-significant different results between the two groups of our study.
This work was the first study about our healthcare system’s experience, and we acknowledge the potential limitations of our research. Different variants of the COVID-19 virus and the availability of facilities and medications may have biased effects, as a confounding factor, on the study’s results, especially mortality outcome. So, studies with larger populations are necessary.
Conclusion
Although the current study is based on a small sample of participants, the findings suggest differences in some parameters, especially underlying comorbidities between the STEMI patients with and without COVID-19 infection who were referred to our medical center during the first 6 months of the pandemic but there was no difference in mortality.
Ethical Considerations
Compliance with ethical guidelines
The protocol of the study was approved by the Institutional Review Boards of the Ethics Committee of Shahid Beheshti University of Medical Sciences (IR.SBMU.RETECH.REC.1399.671). The written informed consent was obtained from each patient before enrollment in the study.
Funding
This research received no specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Authors' contributions
Study design: Roxana Sadeghi and Fatemeh Omidi; Investigation and drafting of the proposal, data interpretation, writing the original manuscript, review and editing: Roxana Sadeghi and Rezvan Hassanpour; Data collection: Fatemeh Omidi and Masoomeh Raoufi; Data analysis: Rezvan Hassanpour; Final approval: All authors.
Conflict of interest
The authors declared no conflict of interest.
References
The novel coronavirus disease 2019 (COVID-19) emerged in Wuhan, China, in December 2019, rapidly evolving into a global pandemic. During the COVID-19 pandemic, the incidence of cardiovascular diseases, including acute coronary syndromes (ACS), stress-induced cardiomyopathy, arrhythmias, and myocarditis, increased [1].
Several mechanisms have been proposed for the pathogenesis of COVID-19 in myocardial injuries. These mechanisms include cytotoxic effect and endothelial damage by angiotensin–converting enzyme 2 (ACE-2) receptor expressed in the myocytes, coronary microvascular obstruction owing to hyperinflammation and prothrombotic state, a mismatch of myocardial supply and demand due to cytokine storm, and acute respiratory distress syndrome (ARDS) associated hypoxemia [2, 3].
The COVID-19 outbreak negatively influences admission rates and the reperfusion strategy for patients with ST-elevation myocardial injury (STEMI) worldwide [4]. Declining admission rates of STEMI patients with COVID-19 and a delay in symptom onset to first medical contact or door-to-balloon have been reported in this population [5, 6]. Additionally, the definition and diagnosis of STEMI in COVID-19 cases have been complex and challenging due to factors such as social distancing, lockdown, health care burden due to the COVID-19 pandemic, and unclear diagnosis of heart attack [4, 5].
Objectives
We designed this study to compare the characteristics, management, and clinical outcomes of patients with STEMI with and without COVID-19.
Materials and Methods
Settings and study population
This prospective observational study was conducted on adult patients diagnosed with STEMI at the Imam Hossein Medical Center, affiliated with Shahid Beheshti University of Medical Sciences (SBMU) in Tehran City, Iran, in the first 6 months of the pandemic, spanning from February 2020 to August 2020.
Assessments
All enrolled patients were evaluated for COVID-19 infection based on reverse transcription polymerase chain reaction (RT-PCR), typical clinical features, and computerized tomography (CT) scan results. Also, STEMI was defined according to the universal definition of myocardial infarction (MI) [7]. All infected patients were managed according to standard treatment protocol based on the updated World Health Organization (WHO) guideline treatment.
Patients were divided into two groups: COVID-19-positive and COVID-19-negative. Then, they were monitored during hospitalization and 6 months after discharge by telephone call. The study data, including baseline characteristics, comorbid risk factors, drug history, clinical and laboratory data, and outcomes, were recorded and compared between the two groups.
Statistical analysis
All statistical analyses were performed using SPSS software, version 21 for Windows (SPSS Inc., Chicago, IL, USA). A P<0.05 was considered statistically significant.
Quantitative data were tested for normality by the Kolmogorov-Smirnov test and then compared by the unpaired t and Mann-Whitney U tests for normally and non-normally distributed data, respectively. Qualitative data were analyzed by the chi-squared or Fisher exact test. The data were presented as Mean±SD or median (percentile, Q1, Q3) for normal and non-normal distributed quantitative data, respectively, and n (%) for qualitative data.
Results
During the period of the study, 131 patients were admitted with STEMI. of whom, 29 patients (22.13%) were diagnosed with COVID-19. None had an RT-PCR result at admission, but they had typical clinical features and CT scan results of COVID-19 infection.
All patients underwent primary angioplasty upon admission, except for 12 patients who initially received thrombolytic treatment (10 and 2 in the COVID-19-negative and -positive groups, respectively; P=0.632), but some hours later, some were candidates for rescue percutaneous coronary intervention (PCI) due to cardiogenic shock (4 patients), persistent chest pain (5 patients) and non-acceptable ST resolution (3 patients).
Most patients were men in two groups of the study (82.35% and 58.62% of COVID-19-negative and -positive, respectively; P=0.007). Also, there was a statistically significant difference between the two groups regarding age, and COVID-19-positive patients were older (63.97±12.54 vs 58.19±10.97 years, P=0.039). Data are presented in Table 1.
The COVID-19-positive patients exhibited a higher prevalence of diabetes (P=0.003) and heart failure (P=0.008). Still, the two groups had no statistical differences for the other comorbid risk factors or drug history (Table 1).
Table 2 presents severe symptoms, echocardiographic and angiographic findings, and some laboratory data during admission.
Erythrocyte sedimentation rate (ESR) and neutrophil count were significantly higher in STEMI patients with COVID-19 infection (P=0.003 and P=0.018, respectively). Instead, lymphocyte count was significantly declined in COVID-19-infected patients (P=0.012).
Whereas STEMI patients with COVID-19 infection were more frequently subjected to coronary artery bypass graft (CABG) surgery during the first admission time (6.7% COVID-19-positive vs 1.96% COVID-19-negative), but this difference was not statistically significant (P=0.173). Furthermore, there were no statistical differences in other complications during hospitalization between the two groups of the present study (Table 3).
In addition, hospital length of stay (HLS) was statistically higher in the patients concomitant with COVID-19 infection (6.64±4.30 vs 4.93±3.59 days; P=0.023).
There were no statistically significant differences between the two groups regarding mortality rate during hospitalization (P=0.095) and 6 months after discharge (P=0.978). During the study period, the overall mortality rate in our setting was 8.82% and 17.24% in COVID-19-negative and -positive, respectively. There was also no statistically significant difference between the two groups (P=0.195). The results are reported in Table 4.
Discussion
This study evaluated clinical characteristics and outcomes in STEMI patients comorbid with COVID-19 infection. We described our healthcare system’s experience of patients presenting with STEMI during the first 6 months of the COVID-19 pandemic. Primary angioplasty is the best-recommended therapy for STEMI, and our setting is an academic center with 247 primary angioplasty and a success rate of more than 95% [8].
Cardiovascular diseases and underlying comorbidities have a high prevalence among COVID-19 patients. Increased risk and severity of COVID-19 infection were also proven in patients with comorbidities [1, 9, 10]. This finding accords with our observations, which showed that the comorbidities, including hyperlipidemia, hypertension, diabetes, chronic kidney disease (CKD), chronic obstructive pulmonary disease (COPD), heart failure, and cerebral vascular accidents (CVA) were common in COVID-19 positive groups. However, only diabetes and heart failure were significantly more frequent in the STEMI patients with confirmed COVID-19.
Furthermore, prior studies have noted that many admitted patients with COVID-19 were men. Evidently, male gender and advanced age were independent risk factors for mortality in the COVID-19-positive population [11, 12]. Consistent with the noted literature, most patients in our study were men, and those infected patients with COVID-19 were older.
Inflammatory markers such as ESR, C-reactive protein (CRP), ferritin, and D-dimer have increased, but lymphocyte levels and neutrophilia are decreasing in COVID-19-infected patients [13]. In addition, Case et al. evaluated natriuretic peptide (NTproBNP) in acute myocardial infarction (AMI) patients with and without COVID-19 infection, which was increased in patients with COVID-19 [9]. In our setting, the patients with COVID-19 had higher levels of WBC, neutrophil, ESR, CRP, ferritin, D-dime, and NTproBNP. However, this study found no significant difference between inflammatory markers except ESR, lymphocyte, and neutrophil.
The present study did not show any significant increase in mortality rate among patients with concomitant COVID-19. This outcome is contrary to that of Case et al., who found a significantly increased mortality in AMI COVID-19-infected patients compared with AMI patients without COVID-19 [9].
The decline in the number of hospital admissions of patients with STEMI because of various reasons such as society’s fear, lockdown, and allocation of high capacity of the hospital for COVID-19 patients during the early months of the pandemic contributed to the small sample size in our study. Therefore, the low sample size and the unequal number in the two study groups are possible reasons for these statistically non-significant different results between the two groups of our study.
This work was the first study about our healthcare system’s experience, and we acknowledge the potential limitations of our research. Different variants of the COVID-19 virus and the availability of facilities and medications may have biased effects, as a confounding factor, on the study’s results, especially mortality outcome. So, studies with larger populations are necessary.
Conclusion
Although the current study is based on a small sample of participants, the findings suggest differences in some parameters, especially underlying comorbidities between the STEMI patients with and without COVID-19 infection who were referred to our medical center during the first 6 months of the pandemic but there was no difference in mortality.
Ethical Considerations
Compliance with ethical guidelines
The protocol of the study was approved by the Institutional Review Boards of the Ethics Committee of Shahid Beheshti University of Medical Sciences (IR.SBMU.RETECH.REC.1399.671). The written informed consent was obtained from each patient before enrollment in the study.
Funding
This research received no specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Authors' contributions
Study design: Roxana Sadeghi and Fatemeh Omidi; Investigation and drafting of the proposal, data interpretation, writing the original manuscript, review and editing: Roxana Sadeghi and Rezvan Hassanpour; Data collection: Fatemeh Omidi and Masoomeh Raoufi; Data analysis: Rezvan Hassanpour; Final approval: All authors.
Conflict of interest
The authors declared no conflict of interest.
References
- Clerkin KJ, Fried JA, Raikhelkar J, Sayer G, Griffin JM, Masoumi A, et al. COVID-19 and cardiovascular disease. Circulation. 2020; 141(20):1648-55. [DOI:10.1161/CIRCULATIONAHA.120.046941] [PMID]
- Chen L, Li X, Chen M, Feng Y, Xiong C. The ACE2 expression in human heart indicates new potential mechanism of heart injury among patients infected with SARS-CoV-2. Cardiovasc Res. 2020; 116(6):1097-100. [DOI:10.1093/cvr/cvaa078] [PMID] [PMCID]
- Yin J, Wang S, Liu Y, Chen J, Li D, Xu T. Coronary microvascular dysfunction pathophysiology in COVID-19. Microcirculation. 2021; 28(7):e12718. [DOI:10.1111/micc.12718] [PMID] [PMCID]
- Baumhardt M, Dreyhaupt J, Winsauer C, Stuhler L, Thiessen K, Stephan T, et al. The effect of the lockdown on patients with myocardial infarction during the covid-19 pandemic-A systematic review and meta-analysis. Dtsch Arztebl Int. 2021; 118(26):447-53. [DOI:10.3238/arztebl.m2021.0253] [PMID] [PMCID]
- Carugo S, Ferlini M, Castini D, Andreassi A, Guagliumi G, Metra M, et al. Management of acute coronary syndromes during the COVID-19 outbreak in Lombardy: The “macro-hub” experience. Int J Cardiol Heart Vasc. 2020; 31:100662. [DOI:10.1016/j.ijcha.2020.100662] [PMID] [PMCID]
- Wang Y, Kang L, Chien CW, Xu J, You P, Xing S, et al. Comparison of the characteristics, management, and outcomes of STEMI Patients presenting with vs. Those of patients presenting without covid-19 infection: A systematic review and meta-analysis. Front Cardiovasc Med. 2022; 9:831143-. [DOI:10.3389/fcvm.2022.831143] [PMID] [PMCID]
- Thygesen K, Alpert JS, Jaffe AS, Chaitman BR, Bax JJ, Morrow DA, et al. Fourth universal definition of myocardial infarction (2018).Eur Heart J. 2019; 40(3):237-69. [PMID]
- Alimohammadzadeh K, Sadeghi R, Maher A, Kazemi MK. Short-term cost-effectiveness of reteplase versus primary percutaneous coronary intervention in patients with acute STEMI a Tertiary Hospital in Iran. Int J Cardiovasc Pract. 2017; 2(3):65-9. [DOI:10.21859/ijcp-020305]
- Case BC, Yerasi C, Forrestal BJ, Shea C, Rappaport H, Medranda GA, et al. Comparison of characteristics and outcomes of patients with acute myocardial infarction with versus without coronarvirus-19. Am J Cardiol. 2021; 144:8-12. [DOI:10.1016/j.amjcard.2020.12.059] [PMID] [PMCID]
- Nishiga M, Wang DW, Han Y, Lewis DB, Wu JC. COVID-19 and cardiovascular disease: From basic mechanisms to clinical perspectives. Nat Rev Cardiol. 2020; 17(9):543-58. [DOI:10.1038/s41569-020-0413-9] [PMID] [PMCID]
- Albitar O, Ballouze R, Ooi JP, Sheikh Ghadzi SM. Risk factors for mortality among COVID-19 patients. Diabetes Res Clin Pract. 2020; 166:108293. [DOI:10.1016/j.diabres.2020.108293] [PMID] [PMCID]
- Rapp JL, Lieberman-Cribbin W, Tuminello S, Taioli E. Male sex, severe obesity, older age, and chronic kidney disease are associated with COVID-19 severity and mortality in New York City. Chest. 2021; 159(1):112-5. [DOI:10.1016/j.chest.2020.08.2065] [PMID] [PMCID]
- Iwamura APD, Tavares da Silva MR, Hümmelgen AL, Soeiro Pereira PV, Falcai A, Grumach AS, et al. Immunity and inflammatory biomarkers in COVID-19: A systematic review. Rev Med Virol. 2021; 31(4):e2199. [DOI:10.1002/rmv.2199] [PMID]
Type of Study: Review Article |
Subject:
General
Received: 2023/04/3 | Accepted: 2023/06/23 | Published: 2023/10/1
Received: 2023/04/3 | Accepted: 2023/06/23 | Published: 2023/10/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |